Multiple myeloma
Here's a case that I have seen -
A 55 year old male, shepherd by occupation, presented to the OPD with the chief complaints of fever (on and off), loss of appetite, headache, body pains, generalized weakness since 2 months, cough since 2 weeks and vomitings and pain abdomen since 2 days.
The patient was apparently assymptommatic 2 months back
Then he developed fever which was insidious in onset, low grade fever, intermittent type.
It is associated with chills and rigors
There are no aggravating factors and the fever was relieved on taking medication
(For which he visited the RMP)
It is associated with generalized weakness, headache (diffuse), neck pain, loss of appetite and weight loss.
It is associated with cough since 2 weeks
It is productive in nature. The sputum is mild in quantity, white in colour, non-purulent, non-blood stained, non-foul smelling.
H/O shortness of breath on exertion
H/O vomitings since 2 days
1 episode/day containing ingested food particles.
Non-bilious, non-blood stained, non-projectile
H/O pain abdomen since 2 days in the right hypochondrium, non- radiating
No H/O loose stools
No H/O chest pain, palpitations, orthopnea, paroxysmal nocturnal dyspnoea
(He visited a hospital in Nalgonda as his complaints didn't subside after taking the medication given by the RMP and then he was referred to Kamineni, Narketpally.)
Past History -
H/O similar complaints 1.5 years back for which he visited a hospital in Nalgonda.
Patient developed fever and generalised weakness 1.5 years ago after which he was diagosed with Anemia and 2 units on PRBCs were transfused.
Not a K/C/O DM, HTN, TB, Epilepsy, Asthma, CVA, CAD
H/O surgery for hydrocele 5 years back
Personal History -
Mixed diet
Decreased appetite
Adequate sleep
Regular bowel and bladder movements
Regular intake of alcohol and beedi (4-5/day) since 35 years.
Patient started consuming alcohol 35 years ago and used to consume about 90ml of whiskey everyday. He started consuming alcohol due to peer pressure and also because he felt relieved after consuming alcohol after work.
The patient stopped smoking beedi 4 years back and he stopped consuming alcohol 4 months back and also stopped going to work due to his health issues (Fatigue)
O/E
Patient is C/C
Poorly built, poorly nourished
Pallor is present

No icterus, cyanosis, clubbing, lymphadenopathy, edema
Vitals -
Temperature - Afebrile
BP - 100/60 mmHg
PR - 120 BPM, Regular
RR - 25 CPM
SPO2 - 94% on RA
CVS - S1, S2 heard, No murmurs
RS - BLAE present, NVBS
P/A - Soft, Non-tender. No organomegaly
CNS - NAD
Investigations-
Day 1-
Hemogram

Bleeding and Clotting Time

ESR

Reticulocyte Count

Peripheral Smear

LFT


RFT


ABG

Chest X-Ray

X-Ray Skull


ECG

USG Abdomen -
1. Right mild pleural effusion
2. Right small kidney with normal echogenicity
HRCT Chest -
1. Moderate to gross right pleural effusion
2. Multilobar consolidations of the right lung, involving upper and middle lobes
3. Passive collapse of basal segments of right lower lobe












Day 2-
Hemogram 
RFT

ABG

Spot Urine Protein/Creatinine Ratio

Sputum for CBNAAT - Positive
(Blood transfusion was done on Day 2)
Day 3 -
Hemogram

ABG

RFT

Chest X-Ray

(Pleural Tap was done)
Serum Protein Electrophoresis

(Blood transfusion was done again on Day 3)
24 Hours Urinary Proteins

24 Hours Urinary Creatinine

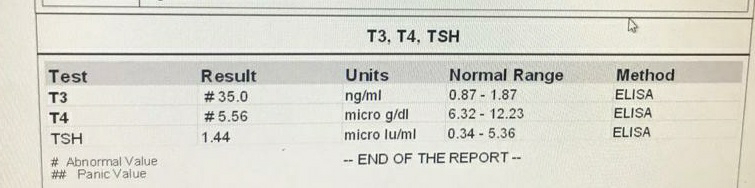
Thyroid Profile
Blood Culture and Urine Culture showed no growth
Sputum (For AFB, Gram's stain and Culture and Sensitivity)

Day 4 -
CBP

ABG

Pleural Fluid LDH

Serum Protein

Pleural Sugar and Proteins

Pleural Fluid Cytology -
Smear studied showed many neutrophils, occassional lymphocytes against a granular eosinophilic proteinaceous background. No atypical cells seen. Features of pleural fluid cytology suggestive of Acute Inflammation.
Bone Marrow Biopsy-
Site - Sternum
Particles - Aspirated 2 ml of blood mixed marrow
Cellularity - Hypercellular M : E ratio = 2:1
Erythropoiesis - Erythropoiesis suppressed with Normoblastic proliferation. Few megaloblasts are seen.
Myelopoiesis - Mild myelosuppression seen with orderly maturation
Megakaryopoiesis - Normal with few hypolobated forms seen
Lymphocytes and Plasma cells -
Lymphocytes - Normal to increased in number
Plasma cells - Plasmacytosis with approximately 30% mature plasma cells seen showing abundant basophilic cytoplasm, eccentric nucleus with characteristic cart wheel chromatin perinuclear hoff binucleate forms, mott cells with russell bodies and occassional plasmablasts seen.
Iron stain - Grade 2 (Normal iron stores)
Impression - Mild suppression of myeloid and erythroid series. Megakaryopoiesis within normal limits. Plasmacytosis seen (30%) showing mature plasma cells. Indicative of most probably plasma cells dyscrasias.










Treatment Given-
1. Inj. Augmentin 0.625 gm/IV/BD
2. Tab. Azithromycin 500mg PO/OD
3. Inj. Pantop 40mg IV/OD
4. Inj. Lasix 20mg IV/BD
5. Plan for 1 unit PRBC transfusion
Diagnosis -
Multiple Myeloma

Please share what was done for this patient in terms of treatment.
ReplyDelete